


INTRODUCTION
The Tokyo 2020 Summer Olympic Games hosted 339 events, the most in Olympic history [1], and the provision of medical support for outdoor athletes faced significant challenges due to the extremely hot conditions and the ongoing coronavirus disease 2019 (COVID-19) pandemic [2]. Nonetheless, a survey conducted by the International Olympic Committee (IOC) revealed a slightly lower incidence of both injuries and illnesses at the Tokyo 2020 Summer Olympic Games compared to the Rio 2016 Summer Olympic Games [3].
Seven new sports were introduced at the Tokyo 2020 Summer Olympics, four of which were classified as extreme sports: surfing, bicycle motocross (BMX), sport climbing, and skateboarding [4]. These sports were specifically chosen to appeal to the interests of the younger generation [4]. When examining the incidence of medical attention required across all sports, sport climbing accounted for 15% of 40 cases, skateboarding for 12.5% of 80 cases, surfing for 10% of 40 cases, and BMX freestyle for 4.2% of 48 cases [2]. Three out of these four sports ranked among the top 10 for incidence rates. Out of the 74 patients who were transported to the hospital, two were from these four new extreme sports [2]. Tanaka et al. [2] focused their study solely on medical care provided at the competition venue, excluding data from the Olympic Village.
Few studies have investigated the epidemiology of injuries sustained during extreme sports activities. The objective of this study was to analyze the characteristics, anatomical locations, and mechanisms of injuries in surfing, BMX freestyle, sport climbing, and skateboarding. These were the first extreme sports to be introduced at the Olympics. The study also aimed to explore their epidemiology.
METHODS
Data
All athletes provided written consent for the use of their medical records at the time of accreditation. The Tokyo Organizing Committee of the Olympic and Paralympic Games' Medical Services Department officially granted permission for data collection, in accordance with the IOC 2020 Consensus Statement on Injury Definition. Furthermore, the Ethics Committee of Kokushikan University approved data utilization (approval No. # 22001).
Injury data were entered and digitally stored by J-SPEED. The collected data included: (1) information from the daily reports of medical operation managers, which detailed the number of cases reported at each location [5]; (2) data from electronic medical records, which included the treatment histories of athletes; (3) medical information sourced from the hospital; (4) data from the main operation center, specifically information obtained from the medical coordination office; and (5) information concerning the final diagnosis from the treating hospital.
These reports were used to gather emergency medical information on injuries and illnesses that transpired at competition venues. The data specifically extracted and consolidated into a single database included: date, location, sport, continent of origin, sex, age, primary complaint, time of occurrence, injury or illness classification, acute or chronic classification, injury mechanism, visit reason, initial vital signs, treatment, diagnosis, and destination medical facilities for transportation. Cases with insufficient data, missing data, duplicates, and data deficiencies met the exclusion criteria and were therefore not extracted. However, if the same athlete required treatment for different diseases and injury sites at various times, each incident was classified and added as a new case.
Participants
A total of 11,420 athletes competed in the Tokyo 2020 Summer Olympics, which took place in 2021. This study focused on 178 of these athletes who participated in four extreme sports: 18 in BMX freestyle, 40 in surfing, 40 in sport climbing, and 80 in skateboarding.
Data analysis
The background and characteristics of four new extreme sports were examined, including factors such as the location of the medical facility where the patient was treated, the patient's age group and sex, the continent where the incident occurred, the timing of the injury or illness, the type of injury or illness, the department that treated the patient, and the reason for the medical consultation. The period and location of the injury or illness occurrence, the mechanism of the injury or illness, and the final diagnosis were also analyzed. Tanaka et al. [2] discussed incidents of accidents, injuries, or illnesses, as well as emergency transport at competition venues, and reported their findings. In this report, duplicate cases were excluded. However, in this study, incidents that occurred at different times and involved different injuries or illnesses were considered separate events. The study also investigated both competition venues and the Olympic Village, and included both orthopedics and physical therapy. As a result, the number of reported cases may have varied.
RESULTS
Background
Out of 178 athletes, 39 required medical attention. This included three from BMX freestyle, eight from sport climbing, eight from surfing, and 20 from skateboarding. There was no significant difference between the sexes, with males comprising 51.3% and females 38.5%. The majority of cases, 61.5%, involved patients in their 20s, while teenagers accounted for 7.7% of all cases; these figures are attributable to the extreme nature of the sport.
Characteristics
Overall
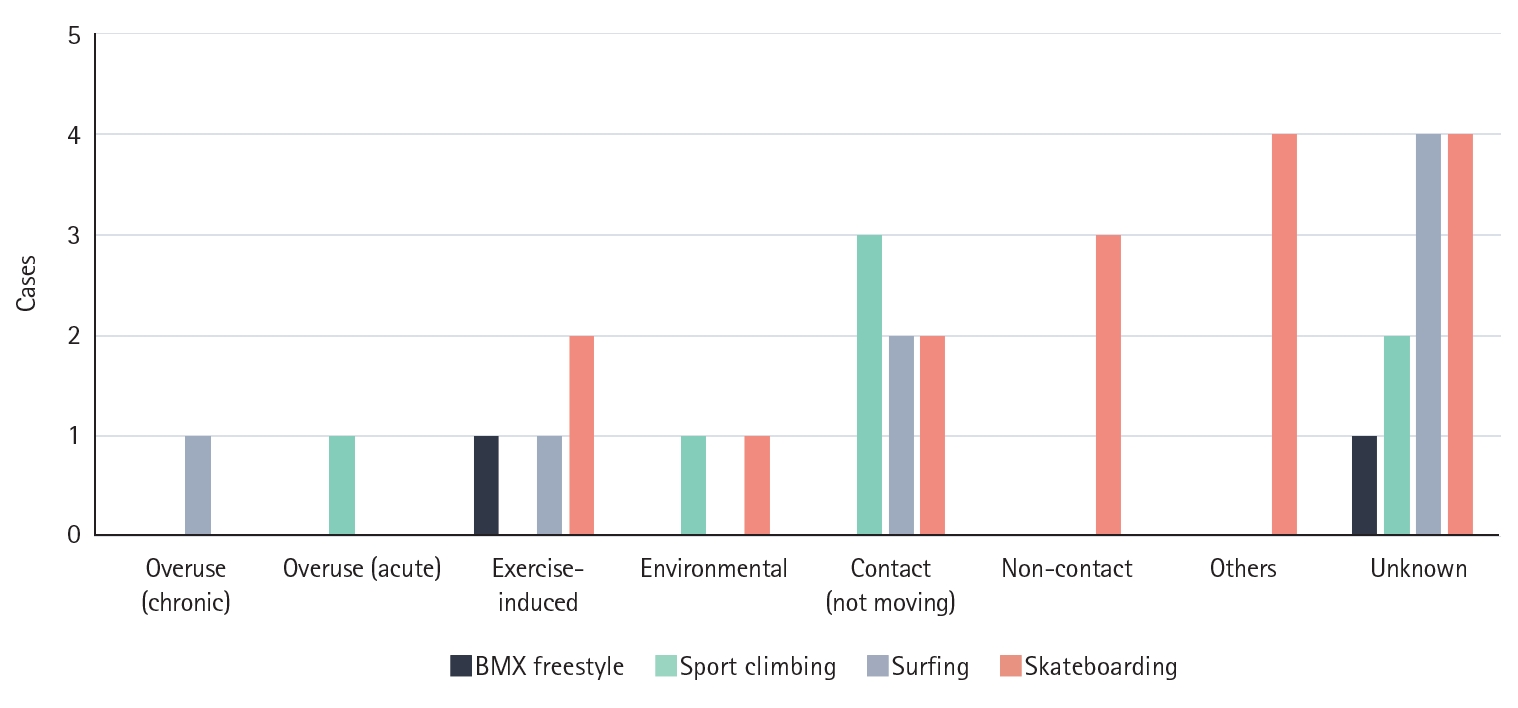
All relevant characteristics are presented in Table 1. Of the total, 59% received treatment at competition venues, while 41% were treated at the Olympic Village. There was a tendency for more acute injuries and illnesses to be reported during the game period compared to the pre-game period. Furthermore, a higher number of visits were made to emergency medical services (46.2%) and orthopedics (30.8%). The primary reason for these visits was injury treatment, which constituted 69.2% of all visits. Only 12.8% of the athletes sought medical treatment, and fewer than 15.4% visited for physical therapy. A total of 35 injuries were reported across four sports, with lower extremity injuries (51.4%) being the most frequently reported anatomical site (Table 2). Contact with an object was the most common injury mechanism (Fig. 1).
BMX freestyle
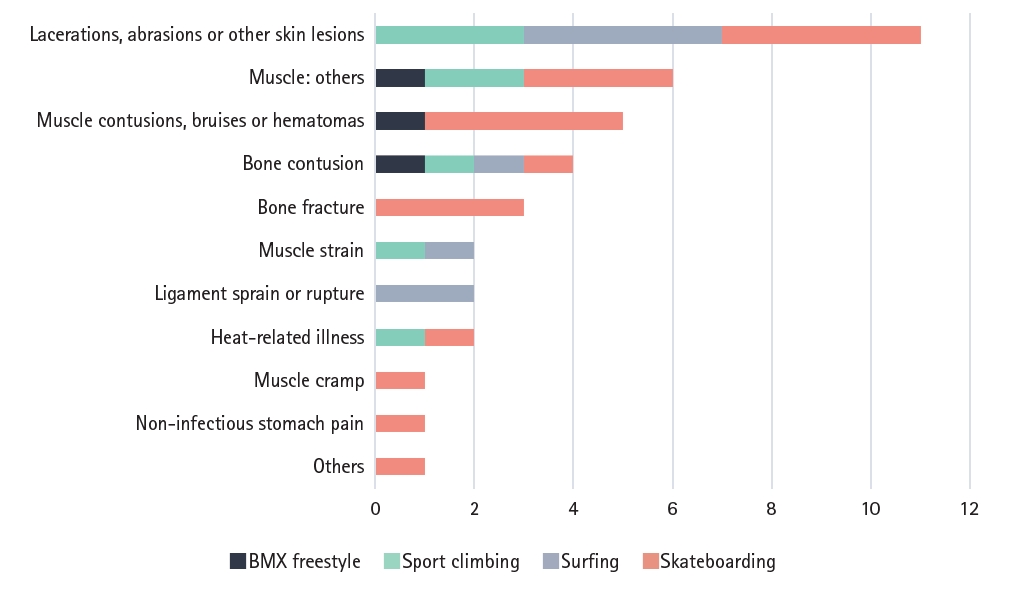
Three patients sustained injuries while participating in BMX freestyle. All these individuals were in their 20s at the time of the competition (Table 1). Two of the injuries (66.7%) involved the upper extremities, necessitating magnetic resonance imaging and, in certain instances, specialist referrals (Table 2). In all cases, the injuries were either muscular or skeletal in nature (Fig. 2).
Sport climbing
Eight cases involving sport climbing were reported, including seven injuries and one illness (Table 1). Three of the injuries were skin lesions, and one was musculoskeletal (Figure 2). Injuries were evenly distributed between the upper (50.0%) and lower extremities (50.0%) (Table 2). The most frequently reported injury resulted from collisions with objects (Fig. 1).
Surfing
All eight reported surfing-related cases involved injuries. The patients visited various departments: two sought help from emergency departments, two from internal medicine departments, one from an orthopedic department, and three from physical therapy departments (Table 1). Among these cases, two were diagnosed with skin injuries caused by rocks, and one was identified as a ligament injury (Figure 2). The mechanisms of these injuries ranged from chronic overuse and exercise-induced injury to contact with objects (Fig. 1).
Skateboarding
Twenty athletes from various extreme sports, including skateboarding, sought treatment at the athlete clinic (Table 1). The athletes represented a wide range of age groups, and injuries were reported across all genders and continents. Of these athletes, 45% required emergency care, while 40% needed orthopedic care. The majority of these visits were due to injuries. Six of these injuries were acute, occurring during practice in the game period, while two occurred during practice in the pre-game period. During the gaming period, 70% of the injuries or illnesses were reported. The majority of these were musculoskeletal injuries or skin lesions. Specifically, there were three cases of distal radius fractures, one case of pelvic contusion, and the remaining cases were reported as contusions or muscle sprains (Fig. 2).
DISCUSSION
During the Tokyo 2020 Summer Olympics, the incidence rate of medical clinic visits at competition venues and Olympic Villages by 178 new extreme sports athletes was found to be notably high. Specifically, 16.7% of these visits were by BMX freestyle athletes, 20% by sport climbing athletes, 20% by surfing athletes, and 25% by skateboarding athletes. Over three-quarters of these new extreme sports athletes required either emergency medical or orthopedic care.
The studies conducted by Soligard et al. [3], which analyzed medical data from the National Olympic Committees and the Olympic Village, and Tanaka et al. [2], which focused on acute injuries and illnesses at competition venues, both reported higher injury rates for newer sports. Soligard et al. [3] found that 22% of injuries occurred in BMX freestyle, 21% in skateboarding, 15% in sport climbing, and 13% in surfing. In contrast, Tanaka et al. [2] reported that 15.0% of injuries in sport climbing and 12.5% in skateboarding required emergency care at the competition venue only, even though the subjects were the same. Soligard et al. [3] reported the total number of athletes who received emergency medical care, orthopedics, physical therapy, otolaryngology, dermatology, ophthalmology, and other departments in both the stadium and Olympic Village. This could potentially explain the difference in findings. The results from both studies suggest that the four extreme sports introduced as new sports at the Tokyo Olympics have relatively high injury and illness rates compared to other Olympic sports.
The overall risk of injury is relatively low for sport climbing [6,7]. Modern sports climbers now compete on walls that are not only steeper but also more three-dimensional than the vertical walls used in the past [8]. Thus, sport climbing is a physically demanding sport that puts significant stress on the arms, legs, hands, and feet. Recent years have seen the emergence of new injuries in sport climbing, including fractures related to heel hook maneuvers [8-10]. In line with previous studies, arm and hand injuries were found to be common in this study. Interestingly, only 2% of athletes in sport climbing reported injuries at the Buenos Aires 2018 Youth Olympic Games [11], in contrast to the 20% injury rate among sport climbers at the Tokyo 2020 Summer Olympic Games.
Surfing, while recognized as a relatively safe sport among extreme sports [12], is not without its risks due to its oceanic nature. Drowning is an inherent risk, and catastrophic injuries to the neck and head can occur due to impact with the seafloor [13]. Fortunately, the athletes participating in the 2020 Tokyo Olympics experienced many minor injuries but were overall safe. Despite the safe conduct reported at the Tokyo 2020 Summer Games, previous studies have indicated that the most common cause of injury is the impact between the surfboard and the seafloor, with a rate of 6.6 injuries per 1,000 hours [13]. Lacerations accounted for approximately 40% of these injuries, followed by sprains/strains, contusions, fractures, and dislocations [13].
Skateboarding is a sport where trauma to long bones and traumatic brain injuries (TBIs) are relatively common [14]. However, during the Olympics, only three fractures were reported, with no instances of TBIs. O'Connor et al. [15] highlighted the inconsistency in the Olympic guidelines, suggesting that the current helmet requirement for those under 18 years of age should also be extended to include those over 18 years.
Research on BMX athletes has predominantly focused on contusions and other skin injuries [16]. Furthermore, fractures and dislocations are relatively uncommon, accounting for only about 10% of all injuries. This suggests that while BMX may appear to be a high-risk sport, it often results in minor injuries [16]. However, a study by Soligard et al. [3] reported a high incidence of injuries during the Tokyo Olympics. In our research, we identified only three cases, two of which were contusions.
The following are some limitations of the study. First, due to the study’s design, we were unable to establish any causal relationships. Second, since this study was confined to Japan, the number of injuries at the Olympic Games in other countries may vary. Third, the administrative and emergency medical systems may have differed significantly from those of previous Games, given that the Olympics took place amidst the ongoing pandemic. Fourth, the methods and perspectives of the National Olympic Committee medical teams vary from country to country, and not all athletes receive the same level of medical care, which could potentially affect the medical records. Lastly, the medical and physiotherapy data from the National Olympic Committee team statistics were not incorporated into these records.
In this study, we analyzed athletes in four extreme sports that were introduced to the Tokyo Olympics. These athletes were examined at both the Olympic Village and competition venues. Of the four sports represented, skateboarding had the highest incidence of medical attention needs. Frequent occurrences of fractures and bruises were observed, underscoring an urgent need for future preventive measures.